

What can your caregiver do to help your baby turn head down?
If your baby is in a breech position after 37 weeks gestation, your caregiver may attempt to guide the baby into the correct position by pushing gently on your tummy while listening carefully to the fetal heart rate with a doppler or by viewing fetal movement with ultrasound (external cephalic version). During this process your doctor is attempting to turn the baby into the head-down, or vertex, position. She would do this by manipulating the baby abdominally. This procedure is common in breech births, it’s usually very safe, and is successful in about 50 to 70 percent of all cases. In terms of pain, it can be a bit uncomfortable. Many women with normal pregnancies may have external cephalic version. Women who can’t have an external cephalic version are women with one of the following:
You have had bleeding (a placenta that is near or covering the opening of the uterus)
You have had a decrease in your amniotic fluid (a low level of fluid in the sac that surrounds and protects the baby)
There is evidence of fetal compromise (a nonreactive nonstress test or an abnormal fetal heart rate)
The umbilical cord is around the baby’s neck (verified by ultrasound)
Prior uterine surgery has been performed
You have had abnormalities of the uterus
An abnormally small baby
Premature rupture of the membranes
Twins or other multiple pregnancy
If you have any of these conditions present, you should speak with your doctor about alternate methods of breech delivery, such as an elective cesarean or a trial vaginal delivery in a hospital.
External cephalic version has some risks, including the following:
Premature labor
Premature rupture of the membranes
A small blood loss for either the baby or the mother
Fetal distress leading to an emergency cesarean delivery
The baby might turn back to the breech position after the external cephalic version is done.
Although the risk of having these complications is small, some doctors prefer not to even try an external cephalic version.
External Cephalic Version: A View of the Procedure



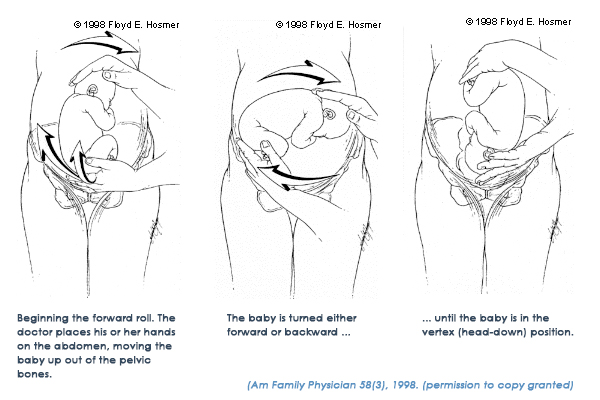
Picture 1 – Beginning the roll. The practitioner places his/her hands on the abdomen, moving the baby up out of the pelvic bones
Picture 2 – The baby is turned either forward or backward …
Picture 3 – … until the baby is in the vertex (head-down) position.
What Can I Expect if my Caregiver and I Decide to Try an External Cephalic Version?
External cephalic version is usually done in the hospital. Before the procedure, you will have an ultrasound to confirm that the baby is breech. Your doctor will also do a nonstress test to make sure that the baby’s heart rate is normal. A tube of blood will be drawn, and an anesthesiologist will be notified, just in case you need to have an emergency cesarean delivery. You’ll be given medicine through a vein in your arm to relax your uterus. This medicine is very safe, with no risk to your baby. While you’re lying down, the doctor will place his or her hands on the outside of your abdomen. After locating the baby’s head, the doctor will gently try to turn the baby to the vertex position. When the procedure is completed, your doctor will perform another nonstress test. If everything is normal, you won’t have to stay in the hospital. If the procedure isn’t successful, your doctor will talk to you about the possibility of having a vaginal delivery or a cesarean section. Your doctor may also suggest repeating the external cephalic version.
What is the Success Rate of an External Cephalic Version?
The success rate of external cephalic version depends on several factors, including the following:
How close you are to your due date
How much fluid is around the baby
How many pregnancies you’ve had
How much your baby weighs
How the placenta is positioned
How your baby is positioned
The average success rate is about 65%. Even if the procedure works at first, there’s still a chance that the baby will turn back around to the breech position. This also depends on the factors listed above.